1. When do you tap a painful swollen joint? When do you obtain imaging before arthrocentesis?
Acute monoarticular arthritis is an inflammatory process involving a single joint that develops over a period of less than 2 weeks. The possible etiologies include infectious, crystalloid arthropathy, trauma, Lyme, and rheumatoid arthritis. The most feared cause is septic arthritis, as failure to diagnose it can lead to significant morbidity and mortality. It can result in permanent disability, with destruction of cartilage in a matter of days. Even treated infections have been associated with an in-hospital mortality rate of up to 15% (Carpenter, 2011). Therefore the main concern in the ED is to diagnose or rule out septic arthritis.
 There are very few published practice guidelines that explicitly indicate when arthrocentesis should be performed from any of the myriad specialties (rheumatology, orthopedics, EM, etc.) that encounter this complaint.
There are very few published practice guidelines that explicitly indicate when arthrocentesis should be performed from any of the myriad specialties (rheumatology, orthopedics, EM, etc.) that encounter this complaint.
EB Medicine’s Emergency Medicine Practice cites the following 4 indications:
- Obtaining synovial fluid for lab analysis
- Draining traumatic tense hemarthroses
- Determining whether a laceration communicates with a joint
- Injecting analgesics and/or anti-inflammatory medications
In regards to the first indication, the authors do not specify when synovial fluid analysis should be done, other than endorsing arthrocentesis whenever septic arthritis is in the differential diagnosis (Genes, 2012).
So when should we consider septic arthritis in the differential? Under what other circumstances should we send synovial fluid? In the setting of a painful swollen joint, the first step is to differentiate a true articular versus periarticular inflammation. Among the latter are bursitis, tendonitis, and cellulitis. These are often associated with pain and swelling in a nonuniform distribution over the joint and limited active range of motion, whereas true arthritis is more associated with generalized pain and swelling, and limitations in both active and passive range of motion (Genes, 2012).
Once you have determined that there is a joint effusion, further physical exam and history may provide clues to the etiology. For example, dry scaly plaques on the skin would suggest psoriatic arthritis, while tophi would suggest gout. However, an important point here is that even if you have a high suspicion for one of these processes, it does not rule out concomitant septic arthritis. Patients with chronic joint disease are actually at increased risk of septic arthritis. Yu, et al. reported 30 cases of concomitant septic and gouty arthritis in their Taiwanese hospital over a 14 year period, underlining the importance of maintaining a high level of suspicion for septic arthritis (Yu, 2013).
So what historical aspects should prompt heightened suspicion? A Dutch prospective study of 5000 rheumatology patients found that the likelihood of septic arthritis increases with the following historical aspects (Kaandorp, 1997):
- Skin infection + prosthesis (+LR 15)
- Joint surgery within past 3 mo (+LR 6.9)
- Rheumatoid arthritis (+LR 3.5)
- Age >80 (+LR 3.5)
- Hip/knee prosthesis (+LR 3.1)
- Skin infection (+LR 2.8)
- Diabetes (+LR 2.7)
Carpenter, et al. conducted a systematic review of 32 trials to determine if there were any physical exam characteristics that altered post test probability of septic arthritis. Exam findings had variable sensitivities across different studies (Carpenter, 2011):
- Pain with motion (100%)
- Limited motion (92%)
- Tenderness (68-100%)
- Effusion (92%)
- Swelling (45-92%)
- Warmth (18-92%)
- Erythema (13-62%)
No studies have looked at clinical gestalt in predicting septic arthritis.
It is generally accepted that x-rays are of little value in the work-up of atraumatic, acute, monoarticular arthritis in the ED. Changes associated with septic arthritis are not seen early. Signs suggestive of other arthritides, such as osteophytes, joint space narrowing, bony erosions, or chondrocalcinosis may be interesting findings but will not rule out septic arthritis or change management. The only utility of plain films is for baseline imaging for the future. CT and MRI are also not indicated, unless there is suspicion of osteomyelitis.
Bottom line: Tap the joint if there is an acute, unexplained, and atraumatic painful joint effusion. If the patient has a history of gout or RA but there is still suspicion for septic arthritis, tap the joint. Consider x-ray but recognize that it will not change your management.
2. In a patient with monoarticular arthritis, do you send any serum labs such as CBC, ESR, or CRP? How do they guide your management?
While it is common to send a serum CBC, ESR, and CRP when suspecting septic arthritis, these tests are not helpful in guiding management. The first issue is that they are very nonspecific. Unfortunately, their sensitivities are also unreliable.
Carpenter, et al. performed a systematic review which analyzed the sensitivities of CBC, ESR, and CRP. Five studies found sensitivities ranging from 42-90% for WBC >10,000. One study yielded a sensitivity of 75% for WBC>11,000. Two studies found sensitivities of 23% and 30% for WBC >14,000. Only two studies calculated likelihood ratios. Jeng, et al. reported a +LR of 1.4 and a –LR of 0.28 for WBC >10,000 (Jeng ,1997), and Li, et al. reported a +LR of 1.7 and a –LR of 0.84 for WBC >11,000 (Li, 2007).
Seven studies looked at various cutoff values for ESR and found sensitivities ranging from 18-95% that had no correlation with the different ESR values being investigated. The same was true of four studies looking at various cutoff values of CRP, with sensitivities ranging from 44-91% in a random fashion. As with WBC, none of the studies that calculated specificities and LRs showed any values that significantly changed the posttest probability of septic arthritis, with the exception of one study, which reported a +LR of 7 if ESR was >100 (Martinot, 2005).
In short, there is no cutoff value of WBC, ESR, or CRP at which the posttest probability of septic arthritis is significantly increased, nor any value below which septic arthritis can safely be ruled out.
Several less commonly sent serum labs have also been investigated. Soderquist, et al. looked at procalcitonin, TNF-a, IL-6, and IL-β and found that all were quite specific but lacked sensitivity (Soderquist, 1998). Two additional studies also analyzed procalcitonin and concluded the same. Therefore, even if these tests yielded results in a timely fashion, none of them would be helpful to send when trying to rule out septic arthritis.
When there is suspicion of gout, serum uric acid is often sent, but again this test is not very sensitive as the value is frequently normal in acute gouty arthritis. Confirmation of Lyme requires IgM and IgG serology, which will not come back while the patient is still in the ED, but may be helpful later and therefore should be sent if suspicion is high (Genes, 2012).
Bottom line: No serum lab will change your management, nor will it rule in or out septic arthritis. Orthopedics and rheumatology will most likely want them regardless.
3. Which synovial fluid studies do you send in order to help make the diagnosis? Which of these rule out septic arthritis?
The gold standard for confirming a diagnosis of septic arthritis is a positive synovial fluid culture; however, it may take several days for cultures to grow, which makes them of little use in the emergent setting. Gram stains may result more quickly and offer the ability to tailor antibiotic treatment. Unfortunately, the yield of gram stains in septic arthritis is only 50-80%. The other synovial fluid labs that are typically sent are of varying utility (Genes, 2012).
Textbooks often cite ranges of synovial WBC values (sWBC) that are associated with normal joints, inflammatory processes, or septic arthritis. It may be more accurate to say that the likelihood of septic arthritis increases with the sWBC, and that for values >100,000 the likelihood is very high. Margaretten, et al. performed a systematic review which looked at 5 studies that each collected data for sWBC cutoffs of 25,000, 50,000, and 100,000. The averaged +LRs were 2.9, 7.7, and 28, respectively, suggesting a significant increase in post test probability for the higher two thresholds. Perhaps the most important point to make is that there is no value of sWBC at which one can safely rule out septic arthritis. Average sensitivities were 77%, 62%, and 29%, respectively, indicating that many patients with septic arthritis do not have exceedingly high sWBC values (Margaretten, 2007).
Four of the above studies also analyzed synovial polymorphonuclear cell counts using the often cited >90% as the cutoff. +LRs ranged from 1.8-4.2, which are not significant values for diagnostic purposes.
It is important to be aware that patients with prosthetic septic joints often present with lower sWBC and sPMN counts. One study that found that values of 1700 and 65% were sensitive and specific (Trampuz, 2004).
Glucose and protein in the synovial fluid do not alter the posttest probability of septic arthritis. Two studies that investigated decreased glucose found sensitivities of 56%-64%, and specificities of 85%. Only one investigated increased protein and reported 50% sensitivity and 47% specificity (Schmerling, 1990; Soderquist, 1998).
One of these studies also investigated synovial LDH and found 100% sensitivity for LDH >250, suggesting that septic arthritis could be ruled out if LDH is <250; however, this is the only study of its kind and was associated with a large number of false positives (specificity 51%) (Schmerling, 1990).
Serum lactate has become one of the most important diagnostic studies sent in suspected sepsis. Likewise, synovial lactate has shown promising diagnostic accuracy in septic arthritis. A recent study showed a +LR approaching infinity for serum lactate > 10 (Lenski, 2014). Several other studies have yielded similar supporting evidence for serum lactate in differentiating septic arthritis from other etiologies such as gout and rheumatoid arthritis. (Brook, 1978; Mossman, 1981; Riordan, 1982; Gobelet, 1984).
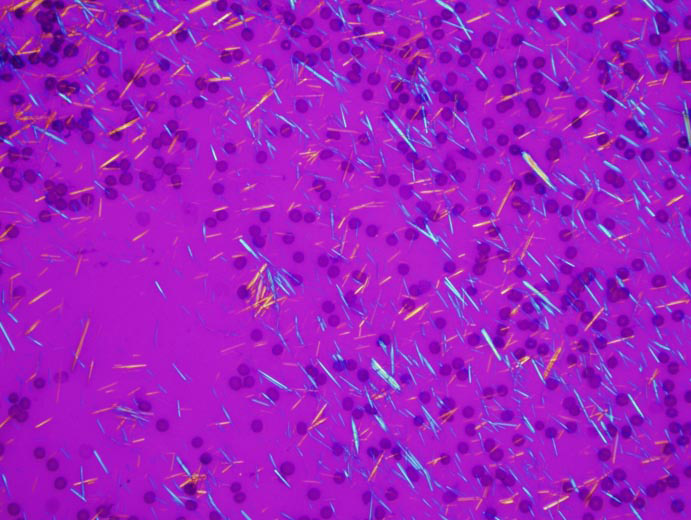
For the diagnosis of gout, the gold standard is the finding of negatively birefringent (MSU) crystals in the synovial fluid (and no organisms). Likewise, the gold standard for pseudogout is rhomboidal, positively birefringent (CPPD) crystals. No cases of either entity have been reported in the absence of the corresponding crystals. However, the finding of crystals does not necessarily explain an acute episode of joint pain, as they can also be found in the synovial fluid of asymptomatic patients (Pascual, 2011).
Bottom line: Synovial fluid culture is the gold standard for diagnosis of septic arthritis. sWBC may be helpful in that a very high value significantly raises the likelihood of septic arthritis (many say 50,000 but 100,000 is much more specific), but a low value does not rule it out. Serum lactate is a promising test that may be available in the future.
4. Do you inject the joint with any medication for symptomatic relief? If so, which medication?
Corticosteroids were the first substances to be injected intra-articularly (IA) for joint pain relief. First described by Hollander in the 1950s, IA steroids have been shown to decrease leukocyte secretion from the synovium as well as neutrophil migration into inflamed joints. This elevates the hyaluronic acid concentration in the joint and therefore the synovial fluid viscosity (Snibbe, 2005). Local injection has been shown to avoid many of the adverse effects of systemic steroids.
Furtado, et al., studied the use of IA steroids in rheumatoid arthritis and found that they gave better results than systemic steroids in terms of side effects, hospitalization, and patients’ subjective reporting of pain and overall disease (Furtado, 2005). Because steroids work on inflamed synovium, results are not as favorable in joint pain caused by weight-bearing forces as in osteoarthritis or sports-related injuries (Snibbe, 2005).
There are several options for steroids. In order of decreasing solubility, which corresponds to increasing duration of effect, they include dexamethasone, hydrocortisone, methylprednisolone, prednisolone, and triamcinolone (Lavelle, 2007).
There are no guidelines for the administration of IA steroids in terms of indication. There are, however, some contraindications. The most important is suspected infection of the joint space or overlying soft tissue. Others include joint prosthesis and bleeding diathesis. There are also concerns about steroid injections producing local adverse effects such as tendon and ligament rupture, soft tissue atrophy, and joint capsule calcification (Snibbe, 2005). As a result, many practitioners will limit the number of injections they give and will not give a repeat dose for at least 3 months (Lavelle, 2007). It is also worthwhile to know that injection of crystalline corticosteroid material can potentially interfere w/ synovial fluid crystal analysis (Parillo, 2010).
Local anesthetic injections are another option for pain relief. Most of the literature supporting their use comes from orthopedic studies looking at the post-operative period, in particular after arthroscopy. Bupivacaine is typically the drug of choice due to its long duration of action. A systematic review of double-blind, randomized, controlled trials comparing IA local anesthetics to placebo showed a statistically significant decrease in both pain scores and additional analgesic requirements (Lavelle, 2007).
The problem with local anesthetics is the potential for cartilage destruction. This has only been found in animals and has not been studied in humans, but concern is high enough that most practitioners limit the number and frequency of injections. There have not been any reports of an ED patient having adverse effects from a single IA dose of a local anesthetic (Genes, 2012), but a study on rats showed prolonged chondrotoxicity after a single IA dose of bupivacaine (Chu, 2010).
Intra-articular opioids (morphine, fentanyl, etc.) have been found to be effective in inflamed tissues, in which the perineurium is disrupted and the opioids have better access to nerve receptors (Lavelle, 2007). Stein, et al., showed that IA morphine actually acted on peripheral receptors rather than systemically by demonstrating that the pain reduction resulting from IA morphine was reversed by injection of IA naloxone (Stein, 1991). Since then the efficacy of IA morphine has been debated, with a myriad of studies investigating its analgesic effects in patients post-op from arthroscopy and ACL repair. One systematic review looked at 19 of these studies and determined that IA morphine had a “mild analgesic effect” (Gupta, 2001). Meanwhile another study found very favorable results for IA morphine in patients with chronic knee pain from osteoarthritis. They actually found that the analgesic effect lasted longer than a week (Likar ,1997).
Other substances that may be injected into painful joints are hyaluronic acid, ketorolac, and clonidine (Lavelle, 2007), but none has been sufficiently studied or is commonly used in the ED.
Bottom line: The best options for intra-articular injections for pain control are steroids, local anesthetics, or morphine. All have been subject to controversy surrounding their efficacies and adverse effects. Steroids should be withheld in suspected infection.