
1.) Do you prescribe ophthalmic topical anesthetics to patients with corneal abrasions who complain of severe pain?
Corneal abrasion is one of the most common acute eye complaints that presents to the ED, accounting for approximately 10% of eye related ED visits (Verma, 2013). The cornea is highly innervated, and even small abrasions can cause significant pain. The use of topical ophthalmologic anesthetics was first documented in 1818 with erythroxylum coca (a cocaine derivative), and is quite effective at blocking nerve conduction in the superficial cornea and conjunctiva, thus eliminating the sensation of pain (Rosenwasser, 1989).
 There are a number of proposed dangers in using topical anesthetics for corneal abrasions. This includes inhibition of mitosis (and subsequent delayed healing) and decreased corneal sensation with the fear that the abrasion will progress to an ulcer without the patient noticing. Additionally, these agents may have direct toxicity to corneal epithelium with prolonged use.
There are a number of proposed dangers in using topical anesthetics for corneal abrasions. This includes inhibition of mitosis (and subsequent delayed healing) and decreased corneal sensation with the fear that the abrasion will progress to an ulcer without the patient noticing. Additionally, these agents may have direct toxicity to corneal epithelium with prolonged use.
These theoretical dangers could potentially lead to keratitis, edema, erosion, and the formation of infiltrates and opacities. These concerns prompted early research of the effects of topical anesthetics on the cornea. The adage that topical anesthetics should not be prescribed to patients with corneal abrasions originated from animal studies and case studies dating back to the 1960’s. Many of the animal studies were done on enucleated rat and rabbit eyes or animal cell preparations. This research may not, for obvious reasons, be applicable to living human subjects.
The earliest human studies date back to the 1960’s and 70’s, and are mostly small case reports of patients using topical anesthetics inappropriately. The first such study was a case report of five patients who used topical anesthetics chronically, resulting in keratitis (Epstein, 1968). All five patients used topical anesthetics for either a prolonged period of time, too frequently, or without physician supervision or proper examination prior to application. In contrast to the inappropriate uses detailed in the case reports, topical anesthetics commonly used to facilitate slit lamp examinations include tetracaine 0.5% or proparacaine 0.5%. A theoretical prescription regimen would be a short course (2-3 days) of a dilute topical anesthetic used only a few times daily (every 4-6 hours as needed).
The next case report condemning the use of topical anesthetics was published two years later, and examined the outcomes of nine patients who misused topical anesthetics (Willis, 1970). Like the previous case reports, this study included nine patients who used topical anesthetics inappropriately: either too frequently, for prolonged periods of time, or without appropriate physician supervision or examination. Of these nine patients, only one patient used the medication in a somewhat reasonable manner (a 46 year old factory worker who used topical anesthetic every two hours for two days), however it is unclear from the paper whether he received a proper slit lamp examination on initial evaluation or was given the drops empirically. When he saw an ophthalmologist two days later, he was diagnosed with anterior uveitis and epithelial erosion, which may have been present at the time of initial injury.
More recent case studies specifically address topical anesthetic abuse and its effects on the cornea (Erdem, 2013; Yeniad, 2010). Types of misuse seen in the literature include using higher concentrations of topical anesthetics, using with excessive frequency, or using for prolonged periods of time. To date, there are no studies that show adverse outcomes from short courses of dilute topical anesthetic with use limited to every 4-6 hours as needed.
There are studies demonstrating the safety of topical anesthetics from the ophthalmology literature. PRK (photorefractive keratectomy) is a type of laser vision correction surgery that involves ablation of a small amount of tissue from the corneal stroma, thus creating an epithelial deficit (similar to a corneal abrasion). In a two-part study, proparacaine was first administered to healthy volunteers in different concentrations to assess anesthetic efficacy (Shahinian, 1997). Dilute (0.05%) proparacaine was then given to healthy volunteers to determine the safety of excessive use. No corneal toxicity was observed. In the second part of the double-blinded study, 34 PRK patients were prospectively randomized into a treatment group (proparacaine 0.05% for one week as needed) or placebo group (artificial tears). Both groups also received oral opioids and topical NSAIDS. Patients in the treatment group reported significantly decreased pain scores, longer duration of pain relief, and decreased opioid use compared to the placebo group.
Another study in the PRK literature looked at post-operative patients given approximately ten drops of tetracaine 0.5% to use as needed (Brilakis, 2000). Patients were re-examined on post-op days 1 and 3. The study found that all of the eyes had healed within 72 hours and use of the tetracaine drops did not prolong time to re-epithelialization.
There are some studies in the emergency medicine literature which support the use of topical anesthetics. One such study was a prospective, randomized controlled trial that included adults with corneal injuries presenting to one of two tertiary emergency departments in Ontario (Ball, 2010). Participants were randomized to receive either proparacaine 0.05% or placebo drops and were followed up by an ophthalmologist on days 1, 3, and 5. All patients were also prescribed topical NSAIDS and oral acetaminophen with codeine, and were told to take the study drops 2-4 at a time as needed. Patients were prescribed 40 mL of drops. The study was small (only 15 patients in the proparacaine group and 18 patients in the placebo group), but showed significantly better pain reduction and decreased opioid use in the proparacaine group. There were no ocular complications or delay in healing in either group.
Another recently published 12-month prospective, double-blinded randomized trial assessed a convenience sample of 116 patients with uncomplicated corneal abrasions (Waldman, 2014). Study participants were randomized to receive either 1% tetracaine or saline every 30 minutes as needed for twenty-four hours. Results showed no complications attributed to topical anesthetics, and no statistically significant difference in corneal healing at 48 hours. To assess pain control, both a visual analogue scale as well as a patient-reported numeric rating scale for overall effectiveness were used. While no difference was seen between the two groups on the visual analogue scale, patients rated tetracaine as having a better overall effectiveness on the numerical rating scale. Although 48-hour follow-up was relatively low (64% in the saline group and 69% in the tetracaine group), the study found that topical tetracaine used for 24 hours was safe and that patients perceived a better overall effectiveness with tetracaine. Both blinding of treatment groups and the pain scores may have been compromised here by the burning sensation that accompanies initial tetracaine application.
Bottom Line: Major EM textbooks still discourage prescribing topical anesthetics for corneal abrasions. In spite of this, there is mounting evidence in the EM literature that topical anesthetics are safe and effective for the treatment of pain in corneal abrasions. It may be reasonable to send selected, reliable patients home with a limited supply of topical anesthetic agents along with strict instructions for return to the ED and 48 hour follow up with an ophthalmologist. Larger randomized, controlled, ED-based studies are needed before the safety of this practice can be fully elucidated and thus, at this time treatment with topical anesthetics cannot be absolutely recommended.
2.) When do you schedule ophthalmology follow up for patients with corneal abrasions?
The cornea functions to protect the eye, filter UV light, and refract light to allow for image formation. To properly refract light the cornea must be completely transparent and thus it is avascular and obtains its nutrients from the aqueous humor, tears, and ambient oxygen. While most corneal abrasions heal quickly and without consequence despite the cornea being an avascular structure, there is potential for complications ranging from infection to ulceration to permanent vision loss, especially if the abrasion is not properly treated.
After a corneal abrasion is diagnosed via slit lamp exam, there are various options for further care. Despite numerous review articles offering various recommendations on the optimal follow up method, there is no evidence-based literature to guide this decision.
Several articles recommend 24-hour follow-up, but don’t specify with whom the patient should follow. A guideline statement from Wilson, et al. recommends that most patients should be re-evaluated in 24 hours and if the abrasion is not fully healed, additional follow-up is needed (Wilson, 2004). It furthermore states that close attention should be paid to contact lens wearers and immunocompromised patients, and that specific ophthalmology referral is recommended for patients with deep eye injuries, foreign bodies unable to be removed, and suspected recurrent corneal erosions. Also, patients with persistent symptoms after 72 hours, worsening symptoms, or vision abnormalities should be referred to an ophthalmologist.
On the contrary, Khan, et al. suggests that patients with corneal abrasions should be seen specifically by an ophthalmologist within 24-48 hours to assess for healing (Khan, 2013). The articles goes on to state that most injuries heal quickly and without infection within 24 hours and that these patients will not need long-term follow-up, with the exception of contact lens users who may need follow-up over the course of 3-5 days.
A review on EM Updates (Strayer, 2009) recommends immediate ophthalmology evaluation if the corneal abrasion is associated with penetrating injury or infiltrate ,and 24 hour ophthalmology evaluation if the abrasion is “high risk,”such as those created by an artificial fingernail or organic matter (which are prone to fungal infections) or contact lens wearers (who are prone to bacterial infections, including pseudomonas). All others can be re-evaluated (not necessarily by an ophthalmologist) in 24 hours.
While most sources recommend at least one follow-up visit within 24-48 hours, some recent articles propose that “small” corneal abrasions (definitions of which range from less than 4mm to less than one fourth of the corneal surface area) which are uncomplicated (i.e., no organic material or contact lens use) in reliable patients with normal vision and resolving symptoms may not require follow-up (Wipperman, 2013).
Do practice patterns reflect these varying recommendations? A nationwide, Canadian survey study that concluded that 88% percent of ED physicians routinely arranged follow-up for their patients with cornal abrasions (Calder, 2004). Most often it was a return to the emergency department (69%) but 45% referred patients to ophthalmologists and 35% referred to the family physician.
Bottom line: Based on expert consensus, it is a reasonable and safe approach to have every patient re-evaluated in 24-48 hours. Those with “high risk” abrasions that you are worried about can be referred to ophthalmology for this follow-up, and others can most likely be re-evaluated by their primary care doctor or told to return to the ED in 24 hours for re-evaluation to ensure proper healing and the absence of infection.
3.) How soon after presentation do you have a patient with floaters see an ophthalmologist?
Floaters are defined as the perception of moving spots in the visual field of one eye. They are usually black or grey in color, and are caused by either light bending at the interface of fluid pockets in the vitreous jelly or opacities caused by cells within the vitreous. They are a very common condition, especially in patients over the age of fifty. In contrast, flashes (which often accompany floaters) can be described as brief repeated sensations of bright light, typically seen at the periphery of the visual field. Flashes are caused by vitreous traction on the retina. Both floaters and flashes are painless (Hollands, 2009; Margo, 2005). Most cases of floaters and flashes (especially when monocular) are of ocular etiology, the most common of which is posterior vitreous detachment (PVD). However, the differential diagnosis also includes retinal tear or detachment, posterior uveitis and other causes of vitreous inflammation, vitreous hemorrhage (which can result from diabetic retinopathy), macular degeneration, ocular lymphoma, intraocular foreign body, TIA, migraine aura, postural hypotension, and occipital lobe disorders. In contrast to ocular etiologies, extra-ocular causes of floaters and flashes are often bilateral and accompanied by other symptoms (Hollands, 2009).
Posterior vitreous detachment is the most common cause of floaters, and occurs in approximately two thirds of patients over age 65 (Margo, 2005). The posterior vitreous is composed mostly of water and collagen. As we age this structure shrinks in size, causing it to detach from the underlying retina. Although most people will develop PVD at some point in their lives, for the majority it will remain benign and without serious consequences. For others, it may progress to retinal tear, which often appears as a horseshoe shaped hole in the retina. Tears allow fluid to enter the sub-retinal space, which then leads to retinal detachment. About 33% to 46% of untreated retinal tears will result in retinal detachment (Hollands, 2009). Retinal detachment causes ischemia and photoreceptor degeneration, which progresses to blindness. If retinal detachment is detected early and surgically corrected, vision loss can be prevented or even restored.
It is difficult to differentiate PVD from retinal tear or detachment based on history alone. Thus, patients who present with unilateral flashes and floaters require a complete eye exam, including visual acuity, pupillary light reflex, visual fields, slit lamp exam of the anterior and posterior segments, thorough inspection of the vitreous using slit lamp, and dilated fundoscopy. Indirect ophthalmoscopy and scleral depression are useful tools (Margo, 2005), but are not routinely performed by emergency physicians and thus, will not be discussed further. A monocular visual field deficit in the affected eye may represent an area of detached retina. A dilated ophthalmoscopic exam can detect a retinal tear (seen as a hole or defect which is often horseshoe shaped) or retinal detachment (which is seen as a billowing or wrinkled retina). Slit lamp exam may reveal vitreous pigment (“tobacco dust”) or hemorrhage, which is suggestive of retinal tear or detachment.
Often, fundoscopic examination is limited in patients with contraindications to mydriatics, significant periorbital soft tissue swelling, or inability to visualize the posterior segment of the eye due to hyphema, lens opacification, or vitreous hemorrhage (Teismann, 2009). In these cases, ocular ultrasound may be beneficial. While the sensitivity and specificity of emergency physician performed ocular ultrasound to detect retinal detachment is beyond the scope of this topic, suffice it to say that ultrasound can be helpful to rule in (but not rule out) the diagnosis.
Since we cannot perform as detailed of an exam as can be done in an ophthalmologist’s office, our role in the ED is to make the diagnosis of probable PVD and to identify patients who are at risk for progression to retinal tear and detachment. Determining this risk will help differentiate patients who require urgent ophthalmology referral from those who can follow up in a less urgent manner. With time, PVD becomes more stable, and patients with floaters and flashes that have remained unchanged for months to years depict a reassuring scenario. In contrast, patients with new onset of floaters and flashes (days to weeks) are more concerning, since the acute phase of tractional forces on the retina makes it prone to developing tears.
In a 2009 meta-analysis, data from 17 different studies regarding patients with acute onset floaters and flashes of suspected ocular origin secondary to PVD demonstrated that 14% were found to have a retinal tear at initial presentation (Hollands, 2009). Besides acute onset of symptoms, other factors found to be predictive of retinal tears included subjective vision reduction and vitreous hemorrhage or pigment (“tobacco dust”) on slit lamp exam. In patients with subjective vision reduction, the prevalence of retinal tears increased from 14% to 45% (likelihood ratio (LR) of 5). The post-test probability of retinal tears in patients with acute onset floaters or flashes (with baseline prevalence of 14%) increased to 62% in patients with vitreous hemorrhage and 88% in patients with vitreous pigment on slit lamp exam. The study also concluded that patients initially diagnosed as having uncomplicated PVD have a 3.4% chance of developing a retinal tear within six weeks. The risk increases with new onset of at least 10 floaters (summary LR 8.1) or subjective vision reduction (summary LR 2.3).
Schweitzer, et al., performed a prospective cohort study looking for predictive characteristics in patients with acute PVD. They found that in vitreal or retinal hemorrhage a large number and/or high-frequency of floaters indicated a high risk for delayed retinal tears within 6 weeks (Schweitzer, 2011). The study was limited by small sample size (99 patients, only two of whom developed delayed retinal tears), however the results make intuitive sense: the more severe the symptoms at onset, the more likely patients are to progress to retinal tears.
Another study reviewed the charts of 295 patients presenting to an eye clinic with complaints of flashes or floaters, and found that 64% had uncomplicated PVD, 10.5% had retinal tears, and 16.6% had retinal detachments (Dayan, 1996). Although the study did identify features that were predictive of retinal tears, including subjective vision reduction and acute onset of symptoms (less than six weeks), a proportion of patients with retinal tears were found to lack these historical factors. The authors recommend routine follow-up visits for patients diagnosed with isolated PVD within six weeks. It should be noted that the study patients presented to an eye specialty clinic and were evaluated initially by an ophthalmologist using tools that are unavailable in standard EDs (i.e. ,indirect ophthalmoscopy with scleral indentation). It could be argued that patients presenting to an ED should be referred for follow-up earlier than the six weeks recommended in this study.
A prospective study of 270 patients with symptomatic, isolated PVD found that 3.7% developed new retinal tears within six weeks. Multiple floaters, a curtain or cloud, retinal or vitreous hemorrhages, and an increase in the number of floaters after initial examination were all found to be predictive of new retinal tears (van Overdam, 2005). Like several others described above, this study identified certain features suggestive of retinal tear that would indicate more urgent ophthalmology evaluation, but did not offer specific recommendations regarding timing of follow-up.
Bottom line: Most cases of floaters or flashes are due to PVD. Although PVD often follows a benign course, a small but clinically significant percentage of patients will develop a retinal tear. Left untreated, the tear can lead to detachment and vision loss. A reasonable approach to managing the patient who presents with floaters or flashes would be as follows (Hollands, 2009):
1.) Start with an exam to rule out obvious retinal tear or detachment seen on fundoscopy or ultrasound. This diagnosis requires emergent ophthalmology consult in the ED.
2.) Patients with monocular visual field loss suggestive of acute retinal detachment (i.e. “curtain of darkness”) or high-risk features for retinal tear (such as subjective or objective vision reduction or vitreous pigment or hemorrhage on slit lamp exam) also require same day ophthalmology evaluation.
3.) In the absence of obvious retinal tear or detachment or aforementioned high-risk features, patients with monocular floaters/flashes thought to be of ocular origin should receive urgent ophthalmology referral (within 1-2 weeks) if symptoms are of acute onset. These patients should be counseled regarding high-risk features, and informed that if any of these symptoms develop, they should return to the emergency department or see their ophthalmologist within 24 hours.
4.) In patients with chronic floaters/flashes that have suddenly increased in number, the case should be discussed with an ophthalmologist to determine the urgency of follow-up.
5.) Patients with chronic, stable PVD should be counseled regarding high-risk features that suggest more urgent ophthalmology evaluation.
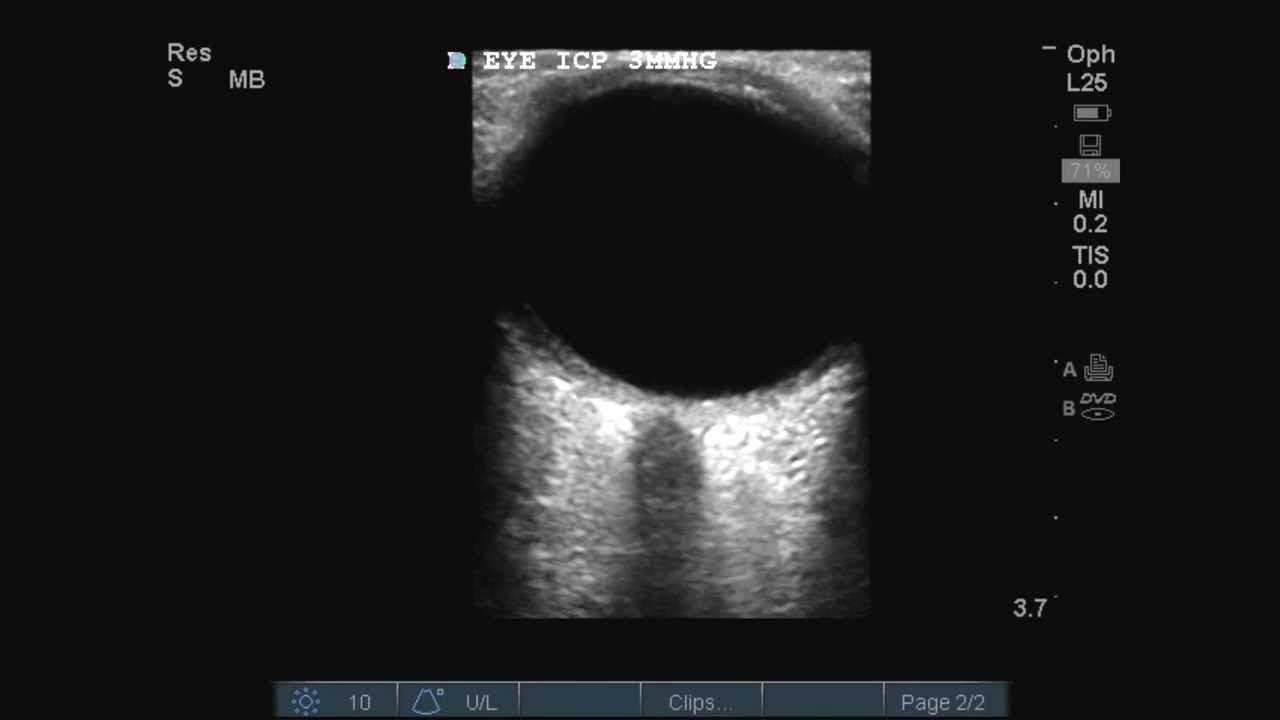
4.) Do you use ultrasound to assess patients for increased intracranial pressure?
Patients who present to the ED with increased intracranial pressure can be quite challenging to evaluate, not only because of their often depressed mental statuses but also because facial trauma and/or patient discomfort may interfere with the ability to perform a fundoscopic exam to assess for papilledema. Ultrasound, which can be done quickly at the bedside in cases where fundoscopy is difficult or impossible, is a useful tool in such circumstances. Multiple studies suggest that emergency physician performed ocular ultrasound to measure optic nerve sheath diameter (ONSD) is fairly sensitive and specific for detecting increased intracranial pressure. One study found that ONSD > 5mm detects ICP > 20 mm Hg with sensitivity of 88% and specificity of 93% (Kimberley, 2008). The prospective, blinded observational study was performed using a convenience sample of patients in the emergency department and the neurological ICU who already had invasive intracranial pressure monitors as part of their care. All ONSD measurements were performed by emergency physicians who were blinded to the ICP monitor data. Another study found slightly improved results when a cutoff of 4.8mm ONSD was used, which was 96% sensitive and 94% specific for ICP > 20 mm Hg (Rajajee, 2011). Like the previous study, the standard criterion was ICP measured via invasive monitoring. A third study compared the ONSD of patients with intracranial hemorrhages requiring ICP monitors in an intensive care unit who were sedated and ventilated to the ONSD of ventilated, sedated control patients without intracranial pathology (Moretti, 2008). A threshold of 5.2mm predicted ICP > 20 mm Hg with 94% sensitivity and 76% specificity.
A prospective study published in Annals of Emergency Medicine found that ONSD greater than 5mm was 100% sensitive and 63% specific for elevated intracranial pressure detected on CT. Furthermore, ONSD > 5mm was 84% sensitive and 73% specific for detection of any traumatic intracranial injury found by CT (Tayal, 2007). Another prospective blinded observational study of a single sonographer who performed 27 ocular ultrasounds in patients with ICP monitors found that ONSD of 5.2mm was 83% sensitive and 100% specific for ICP > 20 mm Hg (Frumin, 2011).
While several papers indicate that ocular ultrasound to measure ONSD does correlate with increased intracranial pressure, much of the literature is based on small observational studies. Large randomized controlled trials are lacking.
While most studies use ONSD as a surrogate for intracranial pressure, a blinded prospective observational study compared point-of-care emergency physician performed ultrasound for optic disc height to both ophthalmology performed dilated fundoscopic exam (primary outcome) and optical coherence tomography (secondary outcome). In contrast to optic nerve sheath diameter, optic disc height refers to the budding of the optic disc into the hypoechoic globe on ultrasound. Results of the study showed that a disc height greater than 0.6mm predicted papilledema with a sensitivity of 82% and specificity of 76%. If the disc height threshold is increased to 1.0 mm, sensitivity decreased to 73% but specificity was 100% (Teismann, 2013).
Much of the evidence for sonographic ONSD measurement comes from head trauma literature. Can ocular ultrasound be used to evaluate non-traumatic etiologies of increased intracranial pressure? Unfortunately, large randomized controlled studies are lacking. A case report of a patient who presented to the emergency department with headache and photophobia who was ultimately diagnosed with pseudotumor cerebri found her ONSD to be 7mm (Stone, 2009). Another paper describes three patients with optic disc swelling due to idiopathic intracranial hypertension, secondary syphilis, and malignant hypertension in which ocular ultrasound revealed elevated optic disc height (Daulaire, 2012).
Two prospective studies evaluated patients presenting to the emergency department who were suspected of having elevated intracranial pressure for various non-traumatic reasons (CVA, SAH, tumor, meningitis, etc.). The first study assessed 26 patients who required CT in the emergency department due to concern for elevated ICP. Prior to CT, all patients received ocular ultrasound to measure ONSD. Using a cut-off of 5mm, ONSD was found to be 100% specific and 84% sensitive for increased ICP on CT. Furthermore, ONSD was 60% sensitive and 100% specific for any acute intracranial abnormality detected on CT (Major, 2011). The second study evaluated fifty patients deemed to be candidates for lumbar puncture due to concern for various diagnoses. Immediately prior to lumbar puncture, ONSD was measured using ultrasound. The mean ONSD for patients with ICP > 20 mm Hg (determined by opening pressure on LP) was 6.66 mm compared to 4.6 mm in patients with normal ICP. Using ROC curves, a cutoff of 5.5 mm predicted ICP > 20 mm Hg with 100% sensitivity and specificity (Amini, 2012).
The literature for ONSD in the evaluation of hydrocephalus seems to be conflicted. In children with VP shunt malfunction, symptoms often overlap with other common childhood illnesses such as viral syndrome or viral gastroenteritis, making timely diagnosis difficult despite the obvious urgency of the situation. Furthermore, CT and MRI are insensitive for shunt malfunction, missing as many as one third of patients. One prospective observational study of pediatric emergency department patients presenting with possible VP shunt malfunction found no statistically significant difference between the ONSD measurements in patients with VP shunt malfunction compared to patients with functional VP shunts (Hall, 2013). Another study showed more promising results: pediatric patients with functioning VP shunts had a mean ONSD of 2.9 mm compared to 5.6 mm in patients with shunt malfunction (Newman, 2002).
Bottom line: Ocular ultrasound can be useful in detecting elevated ICP, especially in the setting of head trauma when fundoscopy is difficult or impossible. Larger studies are needed to confirm these findings.


Always gold. Thanks LITFL
Pingback: Dead Bounceback and Don’t BARF: The FOAMed Report | The Today Online
Pingback: Dead Bounceback and Don’t BARF: The FOAMed Report – Medical 24/7 News
Pingback: EBM Lecture Handout #2: Topical Anaesthetics fo Corneal Abrasions | First10EM